| Myocardial SPECT Lexiscan (40 mCi of Tc-99m-MIBI). There is a small, fixed apicoseptal perfusion defect as well as transient ischemic dilatation with stress. The green arrows point to representative pairs of stress/rest images (stress on top, rest on bottom), demonstrating an increase in the size of the left ventricle with stress (ratio 1.34). |
Tuesday, December 11, 2012
Transient Ischemic Dilatation
Transient Ischemic Dilatation (TID) is an important finding on myocardial perfusion SPECT in that it can be an indication of extensive severe coronary artery disease. The reversible/transient nature of the dilatation corresponds to its ischemic nature, and TID has been associated with a greater risk of future cardiac events. In one study, TID was associated with proximal LAD or multivessel >90% stenosis. In another study a transient dilatation ratio of 1.12 was 60% sensitive and 95% specific for critical multivessel CAD. Despite this, however, these findings are associated with a defect in the myocardial perfusion with stress; it is unclear how severe CAD really is in a patient with TID and no
abnormality in myocardial perfusion.
Monday, December 10, 2012
Pulsed Wave Doppler and Aliasing
Pulsed Doppler is in distinction to continuous wave Doppler.
In continuous wave Doppler, reflectors anywhere in the ultrasound transducer beam contribute to the Doppler signal.
In pulsed Doppler, a piece of the return signal can be selected, thereby only detecting the moving particles at a certain depth and in a particular volume (the "sample volume"). Even though the volume cannot be appreciated on 2D grayscale imaging, it can lead to localization artifact (Doppler signal can be acquired from nearby vessels, not necessarily in the field of view).

In continuous wave Doppler, reflectors anywhere in the ultrasound transducer beam contribute to the Doppler signal.
 |
| From Ref 2 |
In pulsed Doppler, a piece of the return signal can be selected, thereby only detecting the moving particles at a certain depth and in a particular volume (the "sample volume"). Even though the volume cannot be appreciated on 2D grayscale imaging, it can lead to localization artifact (Doppler signal can be acquired from nearby vessels, not necessarily in the field of view).

Sunday, December 9, 2012
The Doppler Equation
Doppler ultrasound interprets the frequency as well as the amplitude of returning sound waves. The Doppler frequency (fD) is defined as the difference between the received and transmitted frequencies of the moving sound wave scatterers (RBCs).
The Doppler angle strongly influences the amount of return signal, with a maximum parallel to the flow (cos 0 = 1), and no signal perpendicular to the flow (cos 90 = 0). The return signal is half strength at 60 degrees (cos 60 =0.5)
---
1. "Introduction to Vascular Ultrasonography" Zweibel and Pellerito, ed. 5th ed. (2005).
 |
| The Doppler equation: f0, initial sound frequency; fr, return sound frequency; v, flow velocity; c, speed of sound. |
The Doppler angle strongly influences the amount of return signal, with a maximum parallel to the flow (cos 0 = 1), and no signal perpendicular to the flow (cos 90 = 0). The return signal is half strength at 60 degrees (cos 60 =0.5)
---
1. "Introduction to Vascular Ultrasonography" Zweibel and Pellerito, ed. 5th ed. (2005).
Saturday, December 8, 2012
Fluoroscopic Landmarks in Femoral Artery Puncture
Although needle access to the femoral artery is most simply performed with palpation, in situations where this is limited (e.g. weak pulses due to atherosclerotic disease? obesity?), ultrasound could easily be used for guidance.
In the old days before readily available high-frequency ultrasound, however, fluoroscopic landmarks were used to help guide puncture in more challenging situations. The most stable landmark is the relationship of the common femoral artery overlying the medial femoral head (below). In one study, the center line of the common femoral artery projected over the medial half of the femoral head in 93% of patients (medial third in 69%, medial to the femoral head in 6%). One source suggests an initial puncture 1 cm lateral to the most medial cortex of the femoral head as the best site for both retrograde and anterograde femoral artery puncture.

This landmark is also useful in that it is above the femoral artery bifurcation and below the inguinal ligament. Puncture of the external iliac artery above the inguinal ligament is associated with significantly higher bleeding complications. Distal SFA punctures are associated with a greater risk of dissection and thrombosis, increased risk of hematoma and pseudoaneurysm, and an increased risk of AVF. A puncture over the femoral head also aids in compression and cessation of bleeding after removing the sheath.
Other points to remember are that calcifications in the arteries can be used to help determine where the lumen is, and that the landmarks mentioned above are critically dependent on normal AP orientation, and deviation from the normal AP orientation can result in a large change in position of the artery relative to the femoral head.
The flip side of recognizing fluoroscopic landmarks is to avoid the vascular structure when making a puncture to access the hip joint space.
Ultrasound guidance is probably prudent in anticoagulated patients with a difficult access approach (obesity, scar, hematoma). The vessel should be punctured as centrally as possible.
---
1. Dotter CT, Rosch J, Robinson M. "Fluoroscopic Guidance in Femoral Artery Puncture" Radiology 127:266-267, April 1978
2. Wacker F, Wolf KJ, Fobbe F. "Percutaneous vascular access guided by color duplex sonography" Eur Radiol. 1997;7:1501-1504.
3. Rutherford's Vascular Surgery. Cronenwett and Johnston. 7th ed. (2010)
In the old days before readily available high-frequency ultrasound, however, fluoroscopic landmarks were used to help guide puncture in more challenging situations. The most stable landmark is the relationship of the common femoral artery overlying the medial femoral head (below). In one study, the center line of the common femoral artery projected over the medial half of the femoral head in 93% of patients (medial third in 69%, medial to the femoral head in 6%). One source suggests an initial puncture 1 cm lateral to the most medial cortex of the femoral head as the best site for both retrograde and anterograde femoral artery puncture.

This landmark is also useful in that it is above the femoral artery bifurcation and below the inguinal ligament. Puncture of the external iliac artery above the inguinal ligament is associated with significantly higher bleeding complications. Distal SFA punctures are associated with a greater risk of dissection and thrombosis, increased risk of hematoma and pseudoaneurysm, and an increased risk of AVF. A puncture over the femoral head also aids in compression and cessation of bleeding after removing the sheath.
Other points to remember are that calcifications in the arteries can be used to help determine where the lumen is, and that the landmarks mentioned above are critically dependent on normal AP orientation, and deviation from the normal AP orientation can result in a large change in position of the artery relative to the femoral head.
The flip side of recognizing fluoroscopic landmarks is to avoid the vascular structure when making a puncture to access the hip joint space.
Ultrasound guidance is probably prudent in anticoagulated patients with a difficult access approach (obesity, scar, hematoma). The vessel should be punctured as centrally as possible.
---
1. Dotter CT, Rosch J, Robinson M. "Fluoroscopic Guidance in Femoral Artery Puncture" Radiology 127:266-267, April 1978
2. Wacker F, Wolf KJ, Fobbe F. "Percutaneous vascular access guided by color duplex sonography" Eur Radiol. 1997;7:1501-1504.
3. Rutherford's Vascular Surgery. Cronenwett and Johnston. 7th ed. (2010)
Friday, December 7, 2012
Lipomatous Hypertrophy of the Interatrial Septum
An occasional incidental finding on Cardiac CT and MR (and transesophageal echocardiography) is Lipomatous Hypertrophy of the Interatrial Septum.
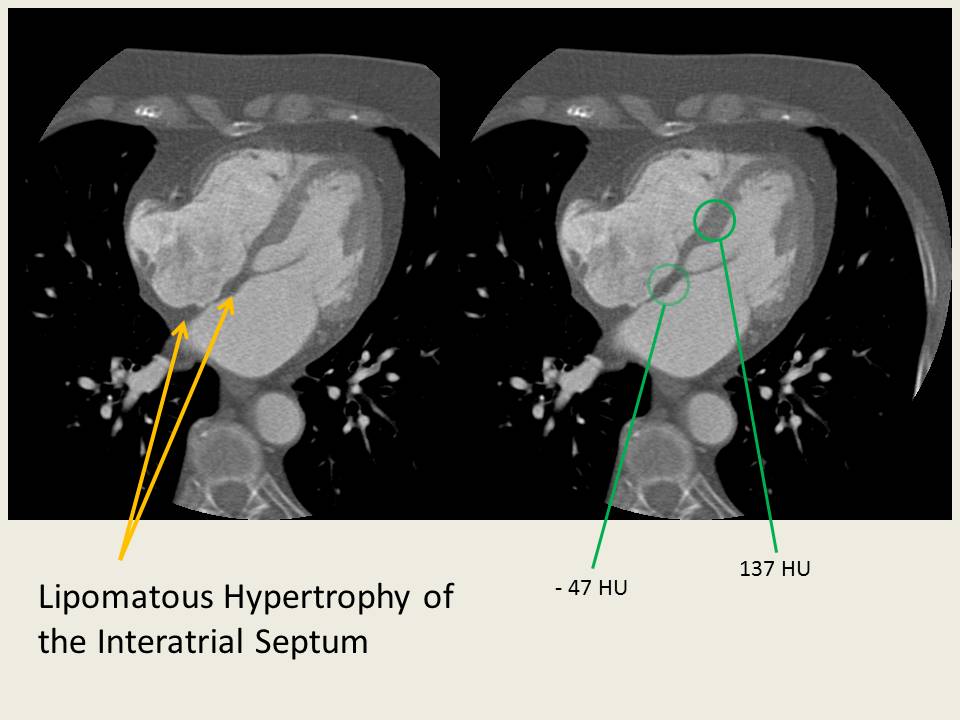 |
| A very mild case of lipomatous hypertrophy of the interatrial septum in this 82Y F being evaluated for a R atrial mass. There was a prominent crista terminalis, but no mass was identified on CT. There's a small amount of fat in the septum as evidenced by the differential attenuation, but relatively little "hypetrophy." Sparing of the fossa ovalis is evident. |