 |
| Conus branch of the RCA. In ~30-50% of people, the conus branch arises off the R coronary sinus. (ref 1) |
Although an acute occlusion of the tiny artery has been shown to result in S-T elevation, another more important role it serves in pathophysiology is that of a route of collateral circulation. The conus has been shown to collateralize with the more distal acute marginal branch in RCA stenosis/obstruction, and collateralize with the LAD in LAD stenosis/obstruction, providing a potentially vital channel.
A fairly common variant origin of the conus artery is off the right coronary cusp, right alongside the right coronary artery (below). This variant led some early anatomists to optimistically name it the "third coronary artery"... although if the fairly common combination of separate origin of the conus artery and RCA off the right coronary cusp were combined with another common variation of a separate LAD and LCx arteries off the left coronary cusp... you could end up with four(!) coronary arteries (although it's really just a different way of looking at the normal two).
 |
| Variations of the conus artery: (top left) Separate origin of the conus (arrow) and the right coronary artery off the right coronary cusp; (top right) Common origin of the right coronary artery and the conus artery (arrow); (bottom left) conus artery (arrow) as a branch of the right coronary; (bottom right) conus artery (arrow) arising from the LAD. (ref 1) |
The conus artery can help to supply the interventricular septum, and an article has noted an enlarged conus artery in a case of HOCM (below). Rarely, instead of originating from the right sinus, the conus has also been found to arise from the left, and in a few case reports of Tetralogy of Fallot, it has even been found to replace the LAD!
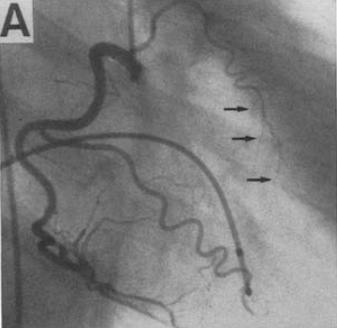 |
| Enlarged conus artery in a patient with Hypertrophic Obstructive Cardiomyopathy (HOCM). (ref 4) |
Whether the conus artery arises independently off the right coronary cusp or as the first branch of the right coronary artery appears to have a significant genetic component. The variant is present in ~50% of Americans, but 38% of Britons, 27% of Pakistanis, and only 10% of the Japanese population.
---
1. Kini S, Bis K, Weaver L. "Normal and Variant Coronary Arterial and Venous Anatomy on High-Resolution CT Angiography" AJR. June 2007. Vol 188:6 pp 1665-1674
2. Matthews RV, Oesterle SN. "Precordial ST elevation with acute conus branch occlusion." Catheterization and Cardiovascular Diagnosis" Vol 17:3 (july 1989) Vol 1:3, pp 180-182
3. Levin DC. "Pathways and Functional Significance of the Coronary Collateral Circulation" Circulation. 1974;50:831-837
4. Sumimoto T, Hamada M, Ohtani T, et al. "A large conus artery in patients with hypertrophic cardiomyopathy" Heart Vessels (1992) 7:52-55
5. "Clinical Cardiac CT: Anatomy and Function" Halpern EJ. 2nd edition, 2011.